Podcast: Play in new window | Download (Duration: 1:10:14 — 48.2MB)
Subscribe: Apple Podcasts | Spotify | Amazon Music
Psychedelic-assisted therapy (PAT) means just that, a medicine used as a tool to deepen the possibilities for healing. It's not the drug, it's the therapy.
NOTE: Find TU listener activities, upcoming meeting etc on FB HERE

Psychedelic-assisted therapy: We don't have to rely on the medicine work to do everything.
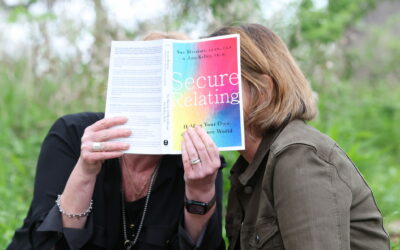
“Plant medicines aren't designed to fix us. They help us recognize our truth and lead us towards the next steps we have to take to heal. This is our work to do. When we become clear with who we are, we can bring our shadow into the light.” – Dr. Dan Engle The use of psychedelics is slowly gaining favor as part of a holistic approach and is radically changing the way we think about therapy and psychiatric medicine. In this episode, Sue Marriott LCSW, CGP discusses the therapeutic use of psychedelics with Dr. Dan Engle, the Founder and Medical Director of Kuya Institute for Transformational Medicine in Austin, Texas. Dr. Engle shares his vision for transformative medicine and how he sees the industry moving forward as it reforms into a transformative model. Tune in and learn more as we explore treatment for various debilitating mental health issues with powerful ancient molecules. Psychedelic-assisted psychotherapy (PAP) refers to professionally supervised use of ketamine, MDMA, psilocybin, LSD and ibogaine as part of a carefully elaborated psychotherapeutic process. Clinical results so far have shown safety and efficacy, even for “treatment resistant” conditions, and far superior effects than traditional therapies alone, or traditional medicines such as antidepressants. In addition, the treatment is short-term and typically has little side effects or risk with careful and adequate screening.

This treatment isn't new, actually, the use of plants to achieve non-ordinary states of mind for wellbeing is ancient. But there has been a renaissance in exploring non-ordinary states as route to healing and the PAP model opens up interesting questions regarding diagnostics and explanation of psychological distress. It may serve to advance novel explanations for mental disorders and their treatment, in a way that considers social and cultural factors, historical adversities, and acute trauma. Show Notes: 00:00:00 Introduction 00:02:11 The Kuya Institute And Community 00:06:41 Sparking An Interest In Psychedelics 00:12:45 Understanding Body And Mind 00:20:03 Exploring The Effects Of Psychedelics 00:28:51 Therapeutic Accessibility Of Psychedelics 00:31:04 Innovating Treatment Models 00:33:21 Ketamine And Its Usage 00:35:11 Ketamine Safety And Psilocybin 00:38:50 Psychedelic States And Safety 00:41:13 The Conscious And Subconscious Mind 00:43:46 The Role Of Facilitators 00:47:34 Tuning Into The Subconscious 00:50:40 MDMA Focused Therapy 00:57:58 MDMA And Altered States 01:01:56 MDMA Side Effects 01:11:26 Contacting Dr. Engle
Complete transcript published below, keep scrolling.
Important Links:
Psychedelics and Neuroplasticity – A Systematic Review Unraveling the Biological Underpinnings of Pychedelics Sept 2021, Psychiatry
- MAPS – Multidisciplinary Association for Psychedelic Studies
- Kuya
- The Second Brain
- My Stroke of Insight
- MAPS Organization
- A Dose of Hope
- Jill Bolte Taylor – Past Episode
- Anatomy of an Epidemic
- Trey Ratcliff – Past Episode
- DrDanEngle.com
- FullSpectrumMedicine.com
- ThankYouLife.org
About Dr. Dan Engle
 Dr. Dan Engle has a unique background in integrative psychiatry, neurocognitive restoration, peak performance medicine and psychedelic research. Dr. Dan unitizes his profound knowledge and experience to help individuals shift from illness and trauma to health and happiness. Dr. Dan’s trans-disciplinary approach focuses on healing all aspects of the mind, body and spirit in order to help individuals achieve optimum health, wellbeing and sustained fulfillment. Dr. Dan is the Founder and Medical Director of Kuya Institute for Transformational Medicine in Austin, Texas; Full Spectrum Medicine, a psychedelic integration and educational platform; and Thank You Life, a non-profit funding stream supporting access to psychedelic therapies. Dr. Dan is the author of The Concussion Repair Manual: A Practical Guide to Recovering from Traumatic Brain Injuries, as well as his new book, A Dose of Hope: A Story of MDMA-Assisted Psychotherapy.
Dr. Dan Engle has a unique background in integrative psychiatry, neurocognitive restoration, peak performance medicine and psychedelic research. Dr. Dan unitizes his profound knowledge and experience to help individuals shift from illness and trauma to health and happiness. Dr. Dan’s trans-disciplinary approach focuses on healing all aspects of the mind, body and spirit in order to help individuals achieve optimum health, wellbeing and sustained fulfillment. Dr. Dan is the Founder and Medical Director of Kuya Institute for Transformational Medicine in Austin, Texas; Full Spectrum Medicine, a psychedelic integration and educational platform; and Thank You Life, a non-profit funding stream supporting access to psychedelic therapies. Dr. Dan is the author of The Concussion Repair Manual: A Practical Guide to Recovering from Traumatic Brain Injuries, as well as his new book, A Dose of Hope: A Story of MDMA-Assisted Psychotherapy.
TYou are invited: JOIN OUR ONLINE COMMUNITY HERE
Support the show AND get access to many cool neuronerd things… including your own private feed that has no ads and tons of extra episodes.
Transcript: Psychedelic-Assisted Therapy With Dr. Dan Engle

Dan Engle MD, Author of Dose of Hope, A Story of MDMA Assisted Psychotherapy
Edited (for clarity):
Welcome aboard, Dr. Dan. We're so happy that you agreed to join us. Thanks for having me on, Sue. It's going to be so nice. We’re going to have an expert who's going to walk us through the state of the state, the state of the art, what's happening with psychedelic medicine, in particular with an eye towards the medicines that are in the queue, psilocybin, MDMA and ketamine, which is the legal one at this point. Would you mind going ahead and jumping in and doing a little warm-up here? Get people oriented to the subject, partly. Say a little bit about yourself, where you are, who you are and a little bit about your background. You've got an interesting story that will lead us right into some of these conversations. I’m happy to do that. Now, I'm in Austin, Texas, back home. I'm from San Antonio and Austin. We’re neighbors. We're right down the road from each other. Next time we're having this conversation, it'll probably be in person. That'd be awesome. I opened up my center, Kuya. It's already been beautiful to see the community build and start. We're wanting to reform and rebirth the new vision for what mental health and mental centers can look like. We have an excellent suite of services. We have a beautiful facility and those two things still sit on top of the fertile, rich foundation, which is our community. The way we've practiced mental health, psychology, psychiatry for the last many decades has been primarily in isolation. When a person goes to see their therapist or their physician, it's usually in isolation. It's not connected to a community. We wanted to reform that. Our community is based on a transformational model where everybody is going through their own process of transformation through their own experience and through their own lens so the community starts to be able to support itself and lift everybody up. When you say community, what do you mean specifically?
You can have people go through mystical states and experiences, whether it's through the veil of a near-death experience or a spontaneous realization.
We have a 10,000-square-foot facility, 2,000 square feet of that are community space. Do you mean the Austin Community or your community of clinicians or patients? All of the above. We see clients from all over the country and the sweetest services because we have a 20% sauna, cold plunges, float tanks, an IV lounge and a tea and tonic bar. We have a lot of associated therapeutics that we can put around the medicine work to support the medicine work doing its job even better. We don't have to rely on the medicine work to do everything. We wanted to build this around a community model. Principally around our clients and our patients coming in the door but also around the recognition that many people who come to see us are going to become, to heal a particular constellation of symptoms depression, anxiety, PTSD, addiction, pain. Our services are very good. We have an excellent track record and we're tracking all of our data. We want to be able to tell them not only the new story of this transformational medicine approach. We want to show the data because the story moves culture but data moves science. When we can show the data and showcase not only the people's transformational experience, we can say, on paper, it makes sense that people would be feeling better because their chronic inflammatory markers are down. Their organic etiology and cause for their longstanding depression has been identified and worked towards resolution whether it's an adrenal issue, a thyroid issue, gut dysbiosis, immune system dysregulation, particularly in the midst of COVID or a variety of other non-organic issues, lifestyle issues, sleep dysregulation, toxicity and the diets. These are all part of the assessment that we have to look at because of this beautiful, complex biopsychosocial spiritual machinery. If we're only looking at the neurochemistry from the standard of care psychiatric model then we're losing the majority of the whole picture. Our suite of services is very good. In regards to the healing orientation, when we put people through our protocols. That same suite of services is very good for people that are also optimizing because if somebody doesn't necessarily have a thing that they want a “heal or fix,” is still good to do a sauna, a cold plunge, float, get IVs, optimize and make sure that the dietary approach that you're using is good for your physiology and your constitution in the right time of the year. The balance of your micro macronutrients. All of this has the opportunity to tell a different story, which we're all in the hairless monkey suit going through our process of transformation, doing it a little bit differently. When we can combine optimization and a healing community then, by osmosis, it allows people that have been stigmatized and labeled with chronic refractory conditions and diagnoses and illnesses that they're always going to have it. It offers us the opportunity to tell a different story. When you say IVs, what is in the IV? What's happening? Is it ketamine? Is it something else? No, we don't use ketamine in an IV administration. We do our ketamine therapy in intramuscular injections and the majority of it. Also some in sublingual or oral trophies or rapid dissolving tablets. IV ketamine has the benefit that you can stop it. If somebody starts having a freakout or bad trip, you can stop it. For us, as a transformational community, I'm curious about that. If somebody has a bad trip, that's excellent information that their stuff is right on the surface. Let's understand that further. Let's create an opportunity with the right set and setting with excellent facilitation to recontextualize a person's ability to lean into that thing that's most uncomfortable because there's so much opportunity for growth there, as you know. It gets into like the mechanism for healing. There are such great results that are coming out of this. As a matter of fact sometimes I get worried. People can become almost evangelical about it. Like, “Everyone, put it in the water.” I worry about that. As a group therapist, if there's only one note being hit, probably something's being missed. However, there are fantastic numbers and effectiveness being shown with these medicines. I am curious because they're all a little different. I want to get into the details of the different psychedelics. To understand, first of all, say you have one person and they have a choice of the different psychedelics. What should they be considering? How do you see them used differently in general? You have, say, the medicines and what are the populations that you feel like each one speaks to? I want to understand how does this works? How is this so effective? Those are a couple of questions there. I've had a long history of intermittent depression. I was probably kindled for that. There's a long history of depression in my family, suicide, real intense dysregulation. That layered on top of half of a dozen severe concussions throughout snowboarding soccer, diving and breaking my neck and all of the different things. I had an organic etiology as well. No one that I saw, even though all my medical training. I got into psychiatry and neurology because I was fascinated by the fields. I was in my neurology training when I had my 6th concussion. My 5th one was when I broke my neck. That was three weeks before medical school started. I started med school in a big halo, which was an awesome orientation to get into psychiatry and neurology. A few years later, in my neurology training, I had my last concussion. Because of the way I hit, I knew it was bad. I put an 8-inch crack in my helmet. There was this internal voice that said, “You crossed the line.” I was like, “That didn't sound so good.” Sure enough, over the coming weeks and months, I started having the severe post-concussive syndrome. I asked my neurology attending physicians. I said, “I got pretty wrecked. Now my sleep is dysregulated. My mood is dysregulated. I can't think. I feel like I'm thinking through the mud. My attention, focus, concentration, short-term memory, shifting sets. All of that. My executive function was lousy.” They all said the same thing. They said, “You had a concussion. You have post-concussive syndrome. Go home, get some rest. We hope it gets better.” I'm like, “That's all you got? Wow.” We have excellent diagnostics and crappy therapeutics. I got in the lab and I wanted to understand neurorehabilitation. That dovetailed with my work with Ayahuasca. It was the first time that I felt my brain come online. I closed my clinic at the time. I moved down to the jungle. I lived in the jungle for a year cleansing with Ayahuasca. I have this understanding and appreciation of the hardware sciences and neurology and the software sciences, psychology. That's essentially what we built at Kuya as a transformational medicine center where we bring both together, the hardware and the software. To answer your last question about IVs, the IV therapeutics that we offer are vitamin and mineral cocktails, peptide therapies. We were working with exosomes and stem cells, particularly for people who have concussive issues and need more of that neurorehabilitation and the accelerated scaffolding for neurologic repair. The FDA has cracked down on biologics and that includes exosomes and stem cells. You must think of stem cells as like seeds for new growth. They start to support regenesis. What was the other thing, exosomes? Exosomes are the fertilizer for that growth. They're their signal messengers but anyway, we can't do that as much. What we do is we use all the therapeutics that are appreciated in the space to be regenerative performance tools. We put that around a person's experience of where they're are orienting to the goals that they have and if they're coming from a healing community then largely, they're going to be desiring to heal from a variety of conditions. If they’re an organic etiology, I also have historically had chronic cytomegalovirus and Epstein-Barr Virus. My titers have been high if I'm stressed and I've done a lot of travel or it's in the winter months. I’m not getting as much vitamin D. When those titers flare, I know I have a higher predilection towards depression. We know those two viral chronic viral infections lead to chronic severe depression. This is an example and because of how I hit, when I dove off a pier and hit a sandbar and my centrally broke C5. I was total upside down. My brain smashed into my skull plate and vice versa too. What happens then is you have pituitary dysregulation and you have an issue that looks like hypopituitarism. It’s primary hypopituitarism because the primary injury is in the pituitary gland but it looks like hypothyroidism, low adrenal glands and low testosterone.
We'll continue to create new therapeutic models to be able to offer the medicine at scale and yet not compromise clinical excellence, efficacy, and safety.
All of that, if you're looking at the labs and you're not looking at the brain, you're going to be like, “All these hormones are low. Let's give you hormones.” That's not the issue. The glands are fine. The brain can't tell those peripheral glands how to work. You have to repair the brain at the central axis. Not to get too complicated but this is an example of where we're going in medicine, which is the appreciation that we're this integrated system. You can't separate the mind from the brain like you can't separate the person from the environment. Gabor Maté’s legendary quote and it's true. We have to understand the complexity of the human organism. That includes looking at our brains, doing brain map systems and taking a good history and physical exams and understanding. Also, there's a great article in Forbes magazine I was reading about the reformation of the entire mental health system. I don't know that we need the entire reformation because it's hardware and software together. What they're saying is maybe many of what we call mental illnesses aren't illnesses at all. They're adaptive responses. There's a lot of truth there. Depression and anxiety can be an adaptive response, especially when we understand what the core issue is, the core wound or the core trigger. That's where medicine comes in. The last thing I'll say about the IV suite is, people can optimize with IV therapeutics. Oftentimes, people who have chronic mental health challenges or psychological constellation of symptoms, oftentimes they have chronic inflammation and that can look like or be stimulated by a variety of different things, including gut dysbiosis, not having awesome diets, GI inflammation. We know in Michael Gershon's book, The Second Brain like the neuroendocrine axis also includes this digestive understanding and appreciation. For example, most of the serotonin is produced and stored in the gut. It gets transferred to the brain. Our serotonin, which we understand like modulates mood. Most of that comes from the gut. If your guts are off, everything's off like sleep. Sleep is off, everything's off. We have to understand how all of this stuff fits together. We recognize, we start giving people IV vitamin mineral cocktails, they start feeling good because it mainlines a lot of the building blocks to optimize neurochemistry and neuro-regulation. All of that then brings us to medicine work. When we understand and we have this hardware framework, the brain and body, physiology framework then we can identify what those organic etiologies are. In complement to that, we want to understand what the software etiologies are, what I would use software meaning like mind, heart and soul. The mind orientation, essentially, if we're thinking about it as a computer, that's where we're receiving all of our belief systems, identification fields, expectancies around who we need to be in the world to get the love that we want. This interpersonal neurobiology starts through that mental filter. We come into life born to bond and what was our early imprinting like. What are our attachment styles like? What was the safety arena? If I look at my own experience, I was born six weeks early. I spent the majority of my first year in and out of the hospital on a respirator because my lungs weren't developed and they didn't have surfactant as a common treatment back then. If I think about my little self and this little incubator thinking, “What the hell is happening? I'm in this sterile environment. I want some warm connection. I want mom. I want the boob. I want all of that connection time.” We can tell a story about what that might look like and what that might mean. All of these are just stories. We try and understand to the best of our ability what's underneath the hood but until you get into work that's able to uncover the subconscious material, we're telling stories and it's all like guesswork. What are the processes that get into the subconscious and the superconscious? Let's say the narrative is mostly a horizontal process but the medicine work is a vertical process. We get into the subconscious, the deep soul-level work and the superconscious like our relationship to God source and spirit and all of that. The experiences offer us that degree of self-examination. In this day and age, the number one in the pole position is psychedelic therapy. It's because it's becoming more appreciated, interesting. The data's super freaking good. When held in the right sentence, setting psychedelic therapy is head and shoulders above the standard of care as far as efficacy rates and safety rates for that matter but it's not new to the extent that we've been exploring psychedelic and transcendent states since we were more hairy monkeys, banging rocks around the campfire. Simon goes back in the foster records a million years. There's evidence that we've been exploring altered states for psilocybin for close to 200,000 years when we transitioned from Homo erectus, Homo sapiens. There may have been part of this exploration and connection with transcendent states through mind-altering substances that helped us get to where we are. We do have biology and a need for transcendence and exploration. Psychedelic therapy is in the new modern context is standing on the shoulder of the evidence and the experiences that have come before. That being said, psychedelic therapies are one way to look deeper under the hood.
Psychedelic-assisted therapy: It's amazing to get under the hood when the ego can just rest its defense mechanisms long enough to have some flexibility and curiosity about actually becoming intimate with those things that we fear the most.
You can get to that level of exploration in altered states through meditation, fasting, Vision Quest, holotropic breathwork, hypnotherapy. I studied hypno for years before I was even aware of psychedelic therapy because it's amazing to get under the hood when the ego can rest its defense mechanisms long enough to have some flexibility and curiosity about becoming intimate with those things that we fear the most. I was a lot. No, you're covering some great stuff. I can feel we're working up to mechanism and how things change. I was speaking to Jill Bolte Taylor. She's the woman who did My Stroke of Insight. She's the neuroanatomist at Harvard that watched her brain shut down. One of the best TED Talks of all time. Twenty-eight million views. Part of what that means is there's something she's saying that people are drawn to. In the middle of the conversation, what happened to her was her left brain, her default mode network went offline. I had the association to psilocybin or to the psychedelics as far as mechanisms. Being able to quiet the conscious, the separateness, the different like, “I am me, you are you,” and all the chatter. You're right. There are different ways of getting at this. We don't want to have head injuries, which by the way, in some of your exploration, I was wondering, “Did you ever look at your high risk-taking behaviors and unconsciously, you may have been acting out with all those head injuries?” I bet I'm not but it is interesting. My sense was that there is something about the language that is like getting around, getting to, allowing. There's something about a release in order to gain access to these other parts of our mind that are not supported in our Western culture that are devalued by our left thinking brain. Not to make it simple as left and right but the idea of the literal, logical, linguistic part of the mind that can think that it knows everything, what I roll at the idea of mysticism and things like that. The mystical is, in my experience, where the magic is. It’s real. You can't measure it but you can't deny it. It was Einstein who was talking about the mystical being the language of consciousness that permeates all life, all experience. We can't be removed from it, nor should we try to. Nor should we try and support medical systems that are divorced from the appreciation of the mystical. In my medical training, we made that wrong. Animism was this old archaic belief of tribal cultures that has no place in modern society. Not only did we shun it, we made it wrong. We developed a pathology around it and it's unfortunate. We're in the midst of trying to rehab all of that. The mystical experience, part of that magic that is a little scary to the medical establishment and paradigm because we haven't been able to quantify it and everybody's experiences are a little bit different. You can have people go through mystical states and mystical experiences whether it's through the veil of a near-death experience or a spontaneous realization. One of my early mentors, he had a clinic that was oriented around people having spontaneous awakenings that they didn't know how to contextualize and what might that look like. He was studying more of an Indian perspective, an Ayurvedic perspective and there's something called the noughties and the energy system from a Chinese medicine perspective that would be the Meridian system. The energy centers in the body all connect to the brain and they go out the top like if you look at the energetic lines of the Earth. It's set up as a tour where we field to like a donut that energy comes in the North and up back around through the South. Our systems are like that too. The energy comes in and it can go up. Sometimes you can have one of these spontaneous awakenings and that can look and feel like people are going crazy because it might mean like now your antenna is tuned to a radio station that you're not familiar with to listen to. It might even be our own internal voice. It could be the voice of our ancestors or of information. Classically, we would call those auditory hallucinations and psychotic. If you have that for too long then you have schizophrenia. If it causes too much discomfort then we're going to label that even with more pathology and a requirement for medication. You might have to stay on the medication for your entire life.
There are a few things that need to be taken into consideration when you think about medicine work, first and foremost is legality and safety.
If you look at, it's Robert Whitaker and the book Anatomy of an Epidemic. Our outcome measures for schizophrenia treatment are worse now than they were a hundred years ago, even in the advent of all of our fancy pharmaceuticals. That's not to say pharmaceuticals don't have their place. Like if somebody's standing on a ledge or if somebody is a danger to themselves or others because they have an experience that they can't manage then yes, let's use those but let's understand that we should only do that while we're looking at the underlying causative factor and reasons for that. All of that to peel it back and say, “In the midst of taking a more whole person perspective,” and what I would say interpersonal or if we talk about like concentric circles. Intrapersonal within, interpersonal between people and transpersonal like our relationship with life and God itself. When we take it from that perspective then we see, we have to appreciate that the medicines have an opportunity to open up each of those spheres. If somebody comes into an engagement or an experience without knowing what's possible then it can freak them out. Even ketamine therapy is done in an IV environment where you try and put people to sleep and ride the default mode network reset and the inflammatory lessening that happens when we clear out the glymphatic system in the brain. The body has a lymphatic system. The brain has a glymphatic system. It might be that ketamine is very good for shunting out some of that intracerebral inflammatory load. It's a great neurologic reset but there's also psychological opportunity. Ketamine, psilocybin and MDMA are this triads now because ketamine is legal. MDMA and psilocybin are going to become legal early to mid-2023. They all have different mechanisms of action, different approaches and different felt experiences. What ketamine is doing is it's offering us the opportunity to solidify our systems, tell a different story and get people in the collective, rehabilitate the propaganda of the war on drugs, which never worked, which was inaccurate and which is unfortunate because it's made many of these medicines wrong. That's taken a while to rehabilitate that entire propaganda approach but it was very effective. Ketamine because it's legal and because it's very convenient, slots into these 60 to 90 minutes sessions because that's about the usual half-life or experience. It's telling people in the medical collective and the lay-person collective that it can be safe to go through a controlled altered state experience. There might be a therapeutic benefit whether it's hitting the brain or in the psyche itself. All of that’s helping to reform our relationship with altered states so that when MDMA and psilocybin become legal, there's more availability, more appreciation and more grassroots demand that these therapeutics not only become legal but they also become available. Now, the way MDMA is set up, when it becomes legal, it's going to be about $14,000 to $16,000 per person to go through treatment. I was going to bring that up about the accessibility issue that certainly has concerns about that. When we can have the grassroots movement to demand that these therapeutics are not only legal but they're also available to the best of our ability to support everybody that needs them, that means we need an entire reformation of the mental health care system. We're in the midst of that. I certainly hope and pray that we are but it’s in my full expectation that's going to happen too because if you look at the trajectory that we've been on. Massive props continue to go out to Rick Doblin and the MAPS Organization for holding the light for so long. All the people are supporting that. They've done what they've needed to do, which is have these patient conversations and relationships with the feds in order to put the evidence in front of the policymakers so that MDMA moves out of schedule one and discuss. That as part of the issue, though because then you have to have these protocols that are measured and have been proven. In order to get into that protocol, we're talking about sometimes multiple therapists hours and before and after. The folks that would be able to access that narrows the scope, unfortunately, partly based on how we have to get it out into the world. You lived overseas. You immersed yourself and there weren’t necessarily those protocols but there was a lot of healing that happened with natural healers I imagine. It's not an unsolvable problem but you still keeping it set in settings, still keeping everything to maximize the benefit of the therapy of it. Not just having a trip but using medicine to do the therapy, to unleash the therapy that you need to do.

Psychedelic-assisted therapy: The mystical experience is the part of that magic that is a little scary to the medical establishment and paradigm, because we haven't really been able to quantify it, and everybody's experiences are a little bit different.
We'll continue to create new therapeutic models to be able to offer the medicine at scale and yet not compromise clinical excellence, efficacy and safety. That's what we do. We innovate. We identify crisis situations, see the opportunity, innovate a solution and continue to iterate towards maximization of its efficacy. We're going to do that with the medicine work. Now, to your point, MDMA support psychotherapy has been done in three sessions, minimum of two. People can opt-in for a third and the vast majority of people do. Let's call it three sessions and you have three psychotherapy sessions before anything happens and after all of that happens and in between the sessions. That's 3 treatment sessions, that's 12 psychotherapy sessions and that's with 2 therapists. You have the time to compensate the therapist for their time. You have the cost of building in the research parameters and observation parameters and the bureaucratic requirements and administrative infrastructure to make sure all that happens in a good, safe way. You can understand why the costs would be so high. There is a ton of money in psychedelic therapy. There are a few companies now that collectively are inching towards two plus billion dollars individually in evaluation. There's no lack of interest, demand and money. It's about understanding, can we move from such a capitalistic orientation towards a service-based orientation to serve the clients that need these treatments. Do that with innovative care and in a reformed medical system that the therapists are reimbursed for what they require for their time that the insurance companies have built this into their model. That small business owners have built this into their models as well. I think we're going to see a lot of innovation, which is on the leading edge of it now. That's the macro. That's the big picture. How about if we go into a little bit more detail. You mentioned ketamine. As a therapist, I’ve worked with people that are doing ketamine treatment and it's interesting. It's not even a psychedelic is that right? Ketamine is not a psychedelic. It’s a dissociative anesthetic. It was used in surgical care, the ‘50s and ‘60s. That was originally in veterinarian medicine and it switched over to human care. It seems less about, at least, how it's been implemented that I can see from my tiny little porthole window. It feels to me like it is more mechanical, like the reset. Sometimes what I'll say is like, the snow path with your skis and if you can shake the globe so to speak and have new paths that. It clears it out. That's great. The psilocybin, there's more of a sense of story that happens with that particular medicine, I believe. Could you say a little bit about the mechanism, about who you know that it's very good for? Sue and I want to know that everybody reading appreciates that there are a few things that need to be taken into consideration when you think about medicine work. First and foremost are legality and safety. Psilocybin and MDMA and some of the other medicines we talk about are not legal. Ketamine is but it's prescription only. It does have addiction potential. Anybody that says ketamine doesn't have an addiction potential doesn't know what they're talking about or they have another agenda because it does. It's understandable and important that it would be a controlled substance. It is being used in the outpatient setting and esketamine nasal spray. We can talk about the efficacy or benefit or approach to that but it's still like opiate pain medications. They have an addiction potential. We know there's an opioid epidemic. There's still a prescription that's schedule three. Not everybody's ready to have a medicine experience. There are few contraindications for ketamine and psilocybin. There are contraindications for MDMA. One of those is Heart Rate Variability, not HRV, in regard to what we're tracking but tachycardia. Elevation of heart rate by 20 to 30 points can happen. Elevation of blood pressure by 20 to 30 points can happen. Anybody who has a severe cardiac history, that needs to be evaluated. That's some of the physical contraindications. You have the psychological contraindications, even though psilocybin is extraordinarily physically safe, there's no LD50, which means you could eat a trash bag of mushrooms. Psilocybins are mushrooms, by the way. You can use psychedelic mushrooms, typically. There are 250 plus psilocybin species in North America alone and 60 to 70 species of those are psychedelic. When we're talking about psilocybin, usually it's cubensis classically in the literature people are talking about. You can eat a trash bag of psilocybin cubensis and not die.
Really good facilitators are conscious of not trying to rescue their clients from their own suffering.
You would probably vomit but there's no LD50 but there's a psychological component and blast them that happens. If people take a heroic dose, usually 1 to 2 grams dried is a mild dose. 3 to 4 grams, more of a moderate dose. Five-plus grams is usually a higher dose. Some people aren't ready to go into the deeper waters. The disclaimer that we want to say is that as you're getting into more specifics, that as you're reading this, that this isn't medical advice. This isn't designed to help you figure out what dose you need to go take. We're talking in general about the effect of it and the research. We do want to get into what you're talking about but the thing that was important was that for everybody to use their discretion and that these are serious, they're complicated medicines that are mostly illegal, probably wherever you're reading, even though that's changing. Having said that with discretion, you were beginning to talk about the effect of psilocybin, in particular, and the therapy. What's the therapy part of it? You can think of it like cars. Cars are tools. They help us go from place to place. I wouldn't want a toddler driving a car because they don't have that skill set, nor psychological development. I don't want many people working with psychedelic states if they don't have the skillset or the psychological development to be able to come intimately into those places that they fear the most. Oftentimes the people say, “I want to have an experience or I want to start the process.” I said, “Great. I appreciate your eagerness or your curiosity at a minimum. Do you have a meditation practice? Do you have an experience of getting scared or up close and personal with something that feels very uncomfortable? If so, how did you manage it? Have you ever been in a float tank? Do you know what a float tank is? Can you be with yourself in the dark alone? If that’s scary, how do you deal with it? When you get triggered or stressed, how do you deal with that?” There's a lot to talk about leading in, how to self-regulate, how to come back to breath, how to recognize when the mind goes on a crazy loop, get curious and recontextualize the interest level and move because the ego typically moves away from the discomfort, particularly in our society. We don't like being uncomfortable and yet, that can be rehabilitated. We can tell a different story. Even the story about somebody getting very uncomfortable and that you were encouraging to be curious about that, rather than to run from it related to the ketamine example from earlier. That is one of the things that's like is it a roar shock that you have experiences and we attribute meaning to them, that's a version or is it that the medicine that it's more direct than that. That it's not just our association to the visual. That it's more the unconscious leading us down the path of the things that we need to address, more personally and specifically. It's well said. We have a conscious mind, a subconscious mind and a superconscious mind. We also have the collective unconscious. There are so many different layers. I would think of conscious like our conversation here is like largely ego-oriented beta way form patterns, the day-to-day. The ego is not bad. It's how we navigate life. We can go below that into the subconscious. What we don't know is immediately available but we can investigate with some leading technologies in therapy and looking under the hood with some of these technologies like medicine work. We can start to get underneath that. We also go into the superconscious and some people might call that like soul or high cell for connection to God. Those are all different, by the way but for examples. There are these layers of knowing, like there are layers of being. When we can start to tell a different story, it's also true that Mike Tyson's coach was fond of saying, like, “Everybody's got a plan until you get punched in the face.” I might tell a person like, “It can be helpful to lean into your fear.” They're like, “Great. I'll do that thing.” We can get into medicine space and they start freaking out because they got punched in the face. That's why I'm there or you're there or the facilitator is there so that we can help them remember like, “Let's slow it all down. Come back to your breath. We were doing that breath training practice. Do you remember that?” That's why I put that whole series in a dose of hope, like walking Alex through the self-regulation breathwork practices before we even got deeper into the weeds of any trauma material. In the midst of the trauma, the ego is going to go, “Holy Crap. Run for the hills or fight flight or freeze.” We go into that old neural pattern. Those are the grooves in the snow. When you have somebody who can catch you right in that moment, lovingly and supportively and say, “Let's take a pause, take a breath, check-in. How do you feel? What do you notice? Can you put a name to it? Can you put association to it? Is there any image? How old do you feel? Where is it coming up in your system? Are there any visual representations, any memories of this?” You start adding the contextual conversation and questions around it.
Psychedelics: Anybody that says ketamine doesn't have an addiction potential doesn't know what they're talking about, or they have another agenda because it does.
Do you do that during the experience or is that something that you're doing like that level of questions? It's such an art and alchemy. It's like Miles Davis said, “The magic is the space between the notes.” Good facilitators are also conscious of not trying to rescue their clients from their own suffering. One of my teachers told me a long time ago because he would see that I want people to feel better. That's why I'm in this work. I know a potential key for humanity is healing. He said, “You also have to check the fact that if you're rescuing somebody from their suffering, you might be robbing them of the greatest teaching.” I was like, “That's important for me to understand.” I've gotten better with the experience of being able to appreciate it like I don't get excited for people suffering because of how it feels. I get excited about the opportunity for them to come into contact with something that they'd been avoiding for so long. I get excited about what that opportunity could serve for them in their lives. All of those questions, I'm checking whether it's appropriate to even ask any question because somebody might be itchy, scratchy, squirmy, an intense experience. I might not do a thing because I want them to linger as long as it takes for it to get ripe. As soon as I see them start to run for the hills then I'm going to ask them to pause. If they're in the midst of and wrestling with, they're coming to terms with it. It’s like in an ayahuasca ceremony. If you know anything about that, medicine is a purgative. It generates a cleansing process. It's like, “I don't want to throw it up. I don't want to stop that process.” Like if somebody has food poisoning, you want them to get it out. You can think about it the same way as poisoning in the psyche. It's old trauma, wounds and programs something that's been festering there and is ready now to be released. Let's not arrest the process. Let's support it and be as a humane, compassionate, directive, guiding when necessary. It's like a midwife supports a natural process. Mom knows cellularly how to deliver this little being. That little being knows cellularly how to move through into the world. The midwives are there to make sure that if a crisis happens then there's intervention and support. I love that analogy because it also speaks to that the body knows what it needs to do. You're also describing a good course of therapy and the therapist’s challenge of hanging back and how massively individualized it is that there's not a formula. In my experience, when I was exploring some of this, for me, to become aware of someone helping was very distracting. I would have to get them out of my brain so that I could have my experience instead of like, “How are they? What’s happening over there?” It's so individual and that's what you're saying. That's the art of it, feeling your way into what is going to serve them and serve this depth of experience so that they can come to see things, come to know things, let go of things, hold on to things in the way with their own little fingerprint have to do or need to do or have the option, have the opportunity to do. I think of it too like a dance. If there's a certain rhythm playing and there's a certain style of dance like flamingo or salsa or two-step or whatever, that has a blueprint but the chemistry shapes how it gets expressed. You have a blueprint in how you perform and offer your psychotherapy. If it's internal family systems or discognitive behavior or DVT, psychodynamic psychotherapy, all the different blueprints and yet there's still the alchemy. That's the magic and some of the mysticism and some of the art. What you're tuning into isn't the conscious mind at all. To know, “Do I speak now or do I not?” that’s not a literal, logical experience that also you are tuning in or even like with the dance that you're describing. Yours is not saying, “Turn now.” It's the magic of the feeling of it. What about MDMA? A lot of people have done it recreationally. They know how to be at a big dance party and have a good time and sweat a lot. What about the therapy related to MDMA? Also, audience, I want to direct you all to a book that he published. We're going to say more about that later. It’s A Dose of Hope. It's in a pill so visually, there's a pill around it. It's an interesting, different book because it was co-written with a pseudo name of a person who went through this experience. It is walking you through detail by detail what it's like and what the healing journey is like. I would highly recommend it. I felt fortunate to be able to get ahold of it and take a look beforehand but it's very interesting. It's exciting.
Usually if somebody is stuck in a loop, they're just looking at kind of a narrow sliver of the entire film of that whole context.
It’s fascinating in how it works. You'd be hard-pressed to find a better molecule for working with PTSD or trauma or psychological defense mechanisms that hold us back from being our most radically true self. That might be a radically wounded self. Let's bring that person, that part, into the center of the circle. Give that part the microphone. Let us get curious about what it has to say. When we look at the efficacy of MDMA-supported psychotherapy, phase one trials, 83% cure rate for chronic severe PTSD. There's nothing like that in psychiatric care, very seldom. That's a lot of very specific attention, attunement and care with the therapists and the folks that are assisting. How did they sort out? What was the medicine versus what is this intense therapeutic experience? Were there focused therapy? It’s MDMA-supported therapy. It's not the MDMA alone. That is important. It's not the trip. The trip opens up the opportunity to get into the deeper part of work. Michael Mithoefer, there were the leads for phase one trials. Their psychological orientation is Internal Family Systems work, IFS parts work. It was Richard Schwartz who wrote this new book called the No Bad Parts. He was the Founder of IFS. I know. We've been after him to bring him onto the show. We can't quite get ahold of him. If anybody knows him, point him our way. That’s a good stag. That’s their zone of genius, doing that IFS work. It doesn't have to be IFS. It can be a lot of other like body-centered psychotherapy, Peter Levine's work, Hakomi. There's a bunch but the way they provide that IFS and part of our training through the MAPS Organization was to watch them in action. They're Jedis. They know that work well and essentially, it's this radical playground of compassion that invites whatever part is online to have the stage and the microphone and to say whatever it needs to say. If you're working with somebody with chronic severe PTSD, that part is probably a wounded part. It's been hard to access by a person's sheer will. If you were to tell them to go rescue the part of themselves that was horribly traumatized, they may have been trying to do that subconsciously as a part of their PTSD internal process of healing. That's why they've had flashbacks and nightmares. They keep reliving it in order to play it through but they guard against it because the ego defenses are in place also for an adaptive response. Somebody's massive trauma, you need to compartmentalize it. Otherwise, it feels too overwhelming. What does the MDMA do or what's the experience of it? It does three primary things in the brain. It calms the fear center, the amygdala. It increases blood flow and the energetic valence of the prefrontal cortex so you have a better witness perspective and it increases the connection between the prefrontal cortex and the hippocampus. Not only do you have a better witness, you have a better memory of the full context of the experience. Usually, if somebody is stuck in a loop, they're looking at a narrow sliver of the entire film of that whole context.
Psychedelic-assisted therapy: You'd be hard-pressed to find a better molecule for working with PTSD or trauma or in psychological defense mechanisms that hold us back from being our most radically true self than MDMA.
What you said is important. I know a lot of our audience will be able to track this and understand what you mean. Saying that again sometimes if I can say it back, it means the information has gotten it. You went fast. I didn't quite keep up. I don't know the order but the thing that I got excited about was particularly the hippocampal involvement. The amygdala we get that, we know fear, all that stuff but by stimulating and focusing the prefrontal cortex and the hippocampus and you said that it regulates the fear center so it lowers your fear, it has more focus and clarity. At the same time, the one that got me excited was the hippocampus because the way we talk about it sometimes is the therapist is the hippocampus. We love the hippocampus. We’re pro hippocampus in this community that it strengthens that, it focuses that, it facilitates a connection with the higher minds and the prefrontal cortex. I haven't heard that before. That's new to me. That's exciting. You hit all three. It affects the amygdala, the prefrontal cortex and the hippocampus. Through that, we have less fear, a better witness, better memory. That was the other one. That's exciting too. Better witness also because you're not in it that you're witnessing it and you're able to objectively not make yourself too big. Not make yourself too little but have this loving, compassionate witness. That's one of the things associated, at least in my mind, with MDMA-facilitated therapy is love. You're flooded with oxytocin. I was going to ask you is it oxytocin? You're flooded with oxytocin, which is this bonding hormone. It's the hormone that moms release at times of childbirth and lactating. We're pro oxytocin and pro hippocampus. That's the summary statement of the differential that happens. PTSD, high amygdala, low oxytocin because most of the time when people are traumatized, it depends on their attachment style if they're avoidant or they're anxious. Either case, the oxytocin or the bonding, let's call it the bonding piece. The bonding piece can oftentimes feel unsafe because it can be cravy like, “I need somebody to help me with this thing,” because that part is so traumatized. It wants safety and security. How do we auto-regulate when we're stressed? Some of us lean in and over-attach. Some of us lean out and dissociate or get the distance. We're all going for the same thing, which is safety and security and our attachment.
We only become self-realized when we have brought all of our parts home.
A lot of that will come up through the process. Now, you have this pro relational oxytocin, sea of curiosity and availability, especially when facilitated by somebody who knows how to do this work, like, “This part is now coming back up to the surface. Can we give that part some space some time to say what it has to say? Let's learn about it. Let's get to know it. Let's validate it.” There’s so much healing. That's a little different than psilocybin, is that right? MDMA is interpersonal, between you and I, between anybody in the field and between all my little parts, horizontal like 3D, like I scanned the horizon. MDMA is much of this world’s medicine. Psilocybin is much a vertical medicine because it can go deep into the soul level matrix. Where do you think about where mushrooms grow? They grow under the ground. They grow in the dark. It's a DMT-based molecule. It also goes up to God and you can have these transpersonal, transcendent experiences with it too. It depends on the direction. It can be healing. You don't get many bad trips with MDMA but you can get bad trips of psilocybin. If a person goes too big too fast or it's not in the right set and setting. We should say uncomfortable trips. The bad trips happen. For example somebody took a truckload of mushrooms and they went to a party. Probably not the best setting to do deep work particularly if they've never worked with that medicine or not done a whole lot of personal work before. I know people that take trucks loads of mushrooms and go to parties and have a fine but it's usually because they've kindled that process. They're familiar with altered states. They'd done a bit of their own personal work. I'm not a fan of getting in huge altered states and going to parties anyway because it's a chaotic field. If you're wanting to do deep personal growth work then have a controlled environment that's supportive to that therapy. If you're taking a bunch of alter states medicines and you're going to a party, that's a recreational experience. That's not a therapeutic experience. Not to make either better or worse than the other. It depends on what your intention is. Even the collaboration of what the dose would be is part of the therapy, I believe. They would tend to be a little bit higher than a recreational experience. Is that right? Not necessarily. It depends on who's partying.

If you're wanting to do deep personal growth work, then have a safe controlled environment that's supportive to that therapy to get to layers you haven't experienced yet.
I think of some of my friends who go heavy and hard. They love to play big. I can bless them up for their choice. I know they play safe. If they weren't playing safe, I'd probably be that guy in the stand shaking his finger, like, “You got to watch out,” because it's not just your experience. You're affecting everybody else's field too. It's about the orientation and the intention going in. The intention for recreational is usually to have an ecstatic state. Maybe a joyful process. Typically, much higher likelihood of having a bad trip. In a therapeutic arena, the orientation is growth. That means we welcome the discomfort into the space so we can look at it, learn from it, grow through it, with it and become more whole as a result. People when they are doing recreational experiences and it's haphazard and dangerous, that's a disintegrative process. It's disconnecting them from what we could describe, essentially their more true essence. People going through a therapeutic process, these medicines are integrative because they're bringing all the parts home into a greater experience of wholeness, union, self-compassion, like Maslow's terms, self-realization. We only become self-realized when we brought all of our parts home. One of the exciting things and research is the effect with addiction. I was imagining people reading this and MDMA and psilocybin. Ketamine has the potential for addiction. I wasn't as aware of that. It's still mild compared to its therapeutic potency and valence but it's still important to recognize as a part of the disclaimer. In contrast to the other ones, which I'm not as clear about MDMA but with psilocybin, that's not typically the recreational use. Psilocybin does not have addictive potential. It's anti-addictive. Some people might get cravy about the transpersonal state. MDMA can have a bit more addictive potential. That's part of why it went into schedule one in the early ‘80s because people were using it dangerously. Like raves, parties, dancing all night, not drinking enough water, having electrolyte imbalances, ending up in ER either tripped out or having seizures, like, “There's this big ecstasy thing hitting the market and hitting the road. Let's shut it down as we did with all the other psychedelics.” It can be a bit of a physiologic kindling because you're like, “I could only get to that elevated state by using this medicine. I'm going to keep using that medicine.” You keep chasing the high. There's a letdown too. Especially if people have a predilection towards depression because you go on these high states, high rise and you have this crash on the other side. The ideal therapeutic container has preparation for neurochemistry. You boil up the neurochemistry, add a lot of antioxidants and on the backside, you replenish with the building blocks to re-establish healthy neurochemistry. That's one of the reasons that disclaimer was a while ago. This isn’t just going crazy by any stretch but I do imagine if people have been following along this conversation, I can imagine people getting very excited about this. I hate to gather people and get them excited about something and say, “Sorry,” or whatever. There's nowhere to send. I can't refer you someplace but there's a wider thing. If somebody is excited about this, what next?
Ideally, we would do what we want to do for everybody, which is not just give them a fish, but teach them how to fish so they're not dependent on something exogenous or external.
Unfortunately, we're on the Fed's timeline for the legalization of MDMA. Rick Doblin’s estimate is going to be early to mid-2023. The assignment passed in Oregon as a statewide therapeutic. That was November of 2020. There's still going to be some bureaucratic, administrative heavy lifting to get that implemented but it's in motion. Cannabis went legal medically in California many years ago. They were the first ones to do that. There are going to be a lot of states that now come into pushing for statewide legalization. That's all happening. Ketamine's legal but those are the big ones. You started though, by talking about your clinic. It's not only those medicines that they're like you said, the breathwork, the deep meditation, finding a community that is interested in some of these more mystical states and whole-body healing that you don't necessarily, it's not a medicine. That's why Kuya, we have all those therapeutic sweets. It's amazing to be able to support people getting into medicine work by working in the float tank because they get used to being with their own process. It's easier to start regulating your breath consciously and flotation therapy is also an amazing integration tool for ketamine work. When you put together those things with contrast therapy, sauna and cold plunging, now you have an active experience in a consistent practice of regulating your nervous system because it's the ability and willingness to lean into something that's uncomfortable. Finding your breath through, particularly in the cold plunge. I'm classically not a fan of cold water. I love being in the mountains and I love skiing and snowboarding but I have not classically been a fan of submerging my body in cold water. It's a phenomenal practice. It increases norepinephrine and 500%. Only three minutes, like 40 degrees plus or minus. It doesn't stay up there but as far as an immediate antidepressant effect, cold plunging is better than medication. It is more adaptive and resilience-building than pharmaceuticals. It has this massive anti-inflammatory effect because cryotherapy does that systemically and centrally. When we stack all of these benefits, there's a very specific reason that I put all of those therapeutics into one umbrella because nobody had done that before. That's one of the reasons that we're tracking all our data because we want to be able to tell the news. That's right. That's why I went back to it so that there isn't the frustration of, “Sorry, you're not going to be able to get this.” I went back to the more well-rounded, all these options. One of the things that was told to me at some point was that conferences and if you're a therapist, there's MAPS that are doing training with therapists. There are trials that are happening all over. Anything else you wanted to add? If people are interested in being an MDMA-supported therapist, you have to go through MAPS because they're the ones in right relationship with the Feds and they're scripting and offering the training that they know is important. Rick's been forward-facing in regards to the recognition. We're going to need a lot of therapists trained up because there's no lack of demand. I doubt there's going to be a lack of demand in our lifetimes. Ideally, we would do what we want to do for everybody, which does not give them a fish but teach them how to fish. They're still not dependent on something exogenous or external. They can develop their own resilience, develop their own skills of self-mastery and transformation. These are tools to help people get to that place to live in. That is such an important point because I think that I didn't understand that, as deeply as I could have but I do now. It's a big distinction. In that sense, it's not the event itself. It's that event or that experience that frees you to do your therapy and like EMDR. When you learn some things about how to target particular symptoms that you can begin to almost do that, you can begin to like, “If I was an EMDR, what would be my target that I'm working on?” The same thing. If you were going to have an experience like this, what would your journey be? What would your intention be? What would you want to happen? Whether or not you have that medicine, that's still a good practice. The meditation, the writing, the journaling, taking yourself seriously. I've also heard spotlight consciousness and lantern conscious consciousness and they're both good. It takes some practice, especially with a culture that doesn't support it of moving into lantern consciousness, which I think is a parallel to what you were saying earlier about the transcendental. Many things to do to deepen our connection to the world and to one another and to spirituality with or without these medicines. I had also interviewed Trey Ratcliff. Are you familiar with him? Super interesting guy. He has a non-medicine, it's super hard to explain but basically, it's a 3D video that goes with some meditation apps. If people are interested in that to bring that back up. You have been so generous to share your wisdom and your experience with us. Would you say a little bit about if people are interested in contacting you, what that would look like and where they should find you? Anything else you want to share with folks around your work? Any recommendations? The top of mind these days is Kuya. I've been working on opening the center for years.

Psychedelics: It's really amazing to be able to support people getting into medicine work by working in the float tank because they get used to being with their own process.
You're affiliated with multiple centers, I think. I do medically advise to a variety of centers nationally and globally but this is my baby so to speak and we opened. I’m some super-stoked. It's already showing us the opportunities that we didn't even recognize before. There's this organic process of me, doing my part to listen and to not think that I know where this is going. I know that we've built something beautiful and amazing. I want to be a student of her and this entire unfolding. I will continue to be an educator and advocate for transformational medicine because I do believe that's on the horizon and one of our biggest opportunities in mental health. I don't have all the answers. I am radically continuing to stay in that curiosity field. I wanted to build a center that is of excellence that we can iterate from, bring people too that's part of the community. I want to create more of the consortium and the think tank of collaborators in the space so that we can have these conversations lifting everybody up. It's so fun. How would they find you? Kuya.life. Kuya means love in Quechua. Kuya.life is our center. People can also find me at my website DrDanEngle.com. That has a variety of different podcasts and other educational pieces. FullSpectrumMedicine.com. That's my education advocacy platform specifically for medicine work. I've got a lot of free content on there about integration practices, preparation practices. Our nonprofit, ThankYouLife.org is a funding stream to scholarship people for medicine work that wouldn't be able to afford it themselves. I love that. That's wonderful. I've worried about that. I'm happy. You've got your hands on a lot of different things. I was thinking. You’re still snowboarding. The ground is different. You're going fast. May that continue to happen and what may we have as much fun doing both. Your book, you want to say that as well and where you can get that. A Dose of Hope, it's a story about MDMA-supported therapy. Essentially, a parable narrative to be able to give the reader a first-person perspective of what it's like to go through MDMA therapy without having to go into the doctor's office themselves so to speak. It also is for the clinician too because I wanted to give some core, in my experience, wisdom teachings around facilitating this work but I didn't want it to be drab and bullet point. These are the things to think about with preparation experience and integration. With kids sometimes you sneak the peas under the mashed potatoes. I wanted to get in some of the good teachings but do it in a way that was entertaining and engaging. Thank you so much. I appreciate you spending time with us and sharing this with us. I know people are going to be very interested. This is all about getting better at healing humans and transforming humans.
Want to join us as a Neuronerd but you aren't as into the audio format / podcasting part, we've got you covered. Our original online platform is still going strong! Join us through our original platform – Patreon. Same exact pricing and levels but you get more communication from us via emails on the platform rather than extra episodes in your podcast feed.
Not ready to join us officially, no sweat. But if you are this deep into the shownotes we hope you have gotten something from the wealth of content in our episode library and we'd love it if you made sure you were actually subscribed to the show and if so, by leaving us a rating and review – that is how the how grows, word of mouth and ratings. TKS FRIEND!